



I am not an MIT-trained neurosurgeon

Wheels In — Intro + Opening Thoughts
Are we ignoring a key component of healthcare innovation: physician experience? Attrition is a growing concern among frontline healthcare workers. Many are leaving the field at a time when we’re already facing doctor shortages. Burnout has been blamed on many factors: moral injury, loss of autonomy, EMRs, increasing administrative burden, and constant insurance hassles (i.e., prior authorization, utilization review, and declining reimbursement). While many proposed solutions allow doctors to “practice at the top of their license,” reality rings hollow. Too many fixes aim to subvert doctors, not help them. Is healthcare innovation elevating the doctor's experience or leaving clinicians behind?
Recently, a YouTube video entitled “I Was An MIT Educated Neurosurgeon Now I'm Unemployed And Alone In The Mountains How Did I Get Here?” went viral. In the, at times, raw video, a former neurosurgeon (“Dr. Goobie”) discusses his reasons for leaving medicine after nine years in practice.
This week, I share some thoughts on “I Was An MIT Educated Neurosurgeon…” based on 15 years as an orthopedic surgeon (and blogger) who’s still gainfully employed on the frontlines.
(I’m a William & Mary grad and went to the Medical College of Virginia for med school).

Dem Dry Bones
From the EIC’s Desk
Dr. Goobie’s lengthy video (48 minutes) covers his reasons for leaving medicine after nearly a decade as a neurosurgeon. For clarity, the Massachusetts Institute of Technology (MIT) doesn’t have a medical school or residency program, but the path to becoming a neurosurgeon is long: 14 years from undergraduate education through residency training, plus another one to two years for fellowship. (My own path to becoming a joint replacement specialist also took 14 years). Most doctors start their careers with educational debt well into the six figures, with an average of around $200,000. Given the considerable time and financial investment required to become a physician, quitting medicine is not an easy choice. On top of that, many face real or perceived family pressure to stick it out.
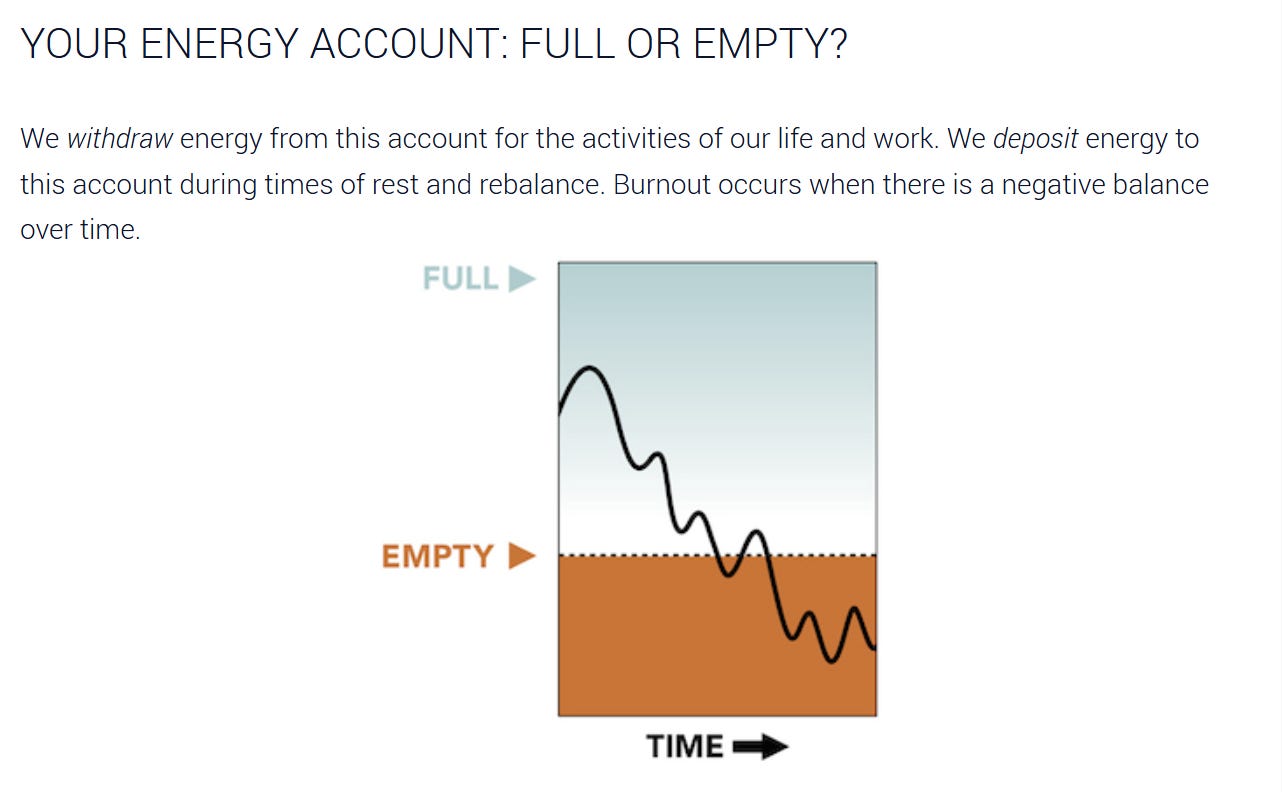
Unfortunately, more doctors are choosing to leave frontline clinical practice. Although he refers to his decision as a mid-life crisis, it’s obvious that Dr. Goobie experienced burnout. The three cardinal symptoms of burnout include:
Exhaustion
Depersonalization
Lack of efficacy
Cardinal Symptoms of Burnout: Exhaustion, Depersonalization, Lack of Efficacy
Dr. Goobie displays evidence of all three symptoms of burnout, especially lack of efficacy. Burnout is often ascribed to moral injury, the concept that our healthcare system constantly forces physicians to act in ways inconsistent with their values. A recent Doximity survey found that 86 percent of doctors are concerned about the future of medicine. Low morale means that 30 percent are considering early retirement. The Clinician of the Future 2023 Education report found that 54 percent of medical students and 62 percent of nursing students view their studies as a steppingstone to careers that don’t involve direct patient care.
Dr. Goobie spends much of the video lamenting that his “perfect” surgeries often resulted in less-than-perfect outcomes. While I’m from the “nothing’s perfect” school of continuous improvement, I empathize with his frustration. Surgery, like most of medicine, is an imperfect science. Objectively well-performed, well-intentioned interventions do not guarantee good outcomes or satisfied patients. The inverse is also true—sometimes “therapeutic misadventures” turn out all right. As we pivot to quality over quantity, this paradox muddies gray waters (and drives clinician angst). Resolving this quandary is essential.
Dr. Goobie attributes inconsistent outcomes to his patients’ underlying health factors. In his experience, patients with healthier lifestyles achieved better outcomes. In fact, such patients often improved without needing surgery at all. Conversely, less healthy patients did worse, surgery or no surgery. Eventually, Dr. Goobie hints that most patients can be healed with lifestyle changes, including more exercise and improved diets.
I have mixed feelings here. First, I absolutely agree that we can and should do a better job offering and rewarding holistic care. Musculoskeletal care in particular would benefit from care pathway design that incorporates lifestyle changes, behavioral modifications, mental health support, improved patient engagement, and adherence to evidence-based practices. Intentionally or not, Dr. Goobie makes a compelling case for condition-specific, value-based care.
However, reality is complicated. “Be Healthy” is medicine’s version of “Git Gud”: an oversimplification of a complex issue. A compelling argument can be made that back pain is overtreated and some (many?) spine procedures are low value. Hip and knee arthritis treatment is less prone to this phenomenon, but certainly not immune. On the other hand, not all surgery can or should be avoided. High-value treatment is doing the right thing for the right patient while optimizing them for a successful outcome. Our mandate is not to think in absolutes but to increase our appreciation of nuance, personalization, and precision. The path isn’t easy, but with persistence, we can “git gud.”
Would Dr. Goobie still be in medicine if he practiced in a sophisticated, supportive system that rose to match the complexity of his patients? Wouldn’t it be great to create solutions that address moral injury while allowing us to take better care of patients? The two seem inextricably linked.
- Ben
Small Incisions
Quick Takes on Timely Topics
Why is Britain’s health service, a much-loved national treasure, falling apart? (CNN)
The goal in highlighting this story is not to engage in schadenfreude but to help push us past the narrative that one approach to healthcare is superior to another. All systems have their pros and cons, and healthcare struggles are worldwide. Let’s stop pitting one against the other in a jingoistic (or anti-jingoistic) attempt to finger-wag. This story is a year and a half old. Things aren’t getting better there (or here). We all have problems. We can all collaborate on solutions.
Many hospitals are nonprofit in name only, and get away with it (Washington Post)
To the surprise of no one. What does surprise (and frustrate) is the apparent unwillingness to offer a solution that has teeth. Meanwhile, we push further down the road of eliminating competition while scratching our heads as things get worse. To paraphrase Logan Roy, healthcare legislation is not for serious people.
Mainstreaming Value-Based Care — Town Hall Ventures
The CY 2025 Physician Fee Schedule may not be all bad, and there’s evidence that maybe, just maybe, CMS is starting to figure out this value-based care (VBC) thing. We tend to think of VBC and fee-for-service (FFS) as mutually exclusive ends of a payment model spectrum. In truth, they exist on a continuum. The final rules include Advanced Primary Care Management codes, quarterly MSSP payments and Health Equity Benchmark Adjustments, and expanded support of telehealth. These proposals allow practices to adopt VBC principles within an FFS framework. Progress? Progress.
Steward Health Care to close Carney and Nashoba Valley hospitals (Boston Globe)
Who's going to buy Steward's remaining Massachusetts hospitals? Physicians can't own hospitals. Legislators have turned up the heat and regulatory scrutiny of private equity and venture capital-backed healthcare (in large part because of Steward's bad apples). Smaller independent community hospitals (of which there are now few) are already struggling financially. Enter large, market-dominant health systems? Or are we willing to think a bit differently and be bold? Otherwise, get ready for more of the same: different wolf, same clothing.
The Gold Standard
Polling the Crowd
The Light Box
Healthcare Visuals
From the Gallery
Amplifying Community Voices

Wheels Out — Signing Off and Looking Ahead
Value-based care absolutely must consider not only patient experience but healthcare provider experience as well. Too many solutions (often offered by outsiders) brush clinicians aside for cost and simplicity’s sake. It’s not a stretch to suggest that many fixes have failed to gain traction or have impact because they fail to appreciate this critical component. At The Surgeon’s Record, we aim to raise awareness of critical issues facing clinicians and amplify doctors’ voices. We all benefit from a system that reduces burnout and keeps more physicians in the game.
On another note, this week The Surgeon’s Record launches our first webinar featuring a discussion between Commons Clinic CEO Nick Aubin and Dean Dalili, CEO of Healthcare’s Most Trusted AI Scribe, DeepScribe (with yours truly moderating). It should be an enlightening discussion between two healthcare innovators (and me).
See you there,
Ben Schwartz, MD, MBA
Editor-in-chief/Senior clinical fellow
Hey Ben, Do you have registration information for the webinar? Thanks.