

Does CMS Hate Specialists?
Part One: The Problem

As a total joint surgeon, I spent most of my career caring for people over 65. In fact, about 70% of my patients were covered by some flavor of Medicare or Medicaid. I lived through the rollout of VBC programs, the elimination of the IPO list, the rise of ASCs, and other attempts by CMS to arbitrage the value of arthroplasty.
I never considered dropping Medicare. Like most specialists, I dutifully played by CMS’ rules — even when they seemed unfair, arbitrary, or self-defeating. When the treadmill sped up, I ran faster. When the rules changed, I adjusted.
Then again, what choice did I have? It’s easier to leave the Mafia than it is to opt out of Medicare. CMS knows this. It has repeatedly called the “opt out” bluff, and docs fold every time.
Joint replacements are among the most successful interventions in the history of medicine. They are life altering for patients and provide tremendous societal benefit — up to $30,000 per patient. To match that level of value, the price of GLP-1s would have to drop 80%. Modern joint replacements last a lifetime. GLP-1s have to be taken forever.
Despite their already high value proposition, CMS is constantly squeezing the margins on joint replacements. Declining reimbursements are one thing. But every newly announced CMMI innovation program seems specifically designed to deemphasize the role of specialists.
Does CMS hate specialists?
Programs like ACCESS, TEAM, ACO LEAD, and the recently unveiled CJR-X consistently treat specialists like followers, not leaders. Why does CMS seem determined to route care around specialist expertise rather than through it? Is this circuitousness the best way to achieve accountability? Do gatekeeping and forced collaboration trade short-term value creation for long-term value erosion?
CMS may or may not hate specialists, but I’d argue it’s grossly misinterpreting their value.
Payment Reality Refresher
I covered the payment picture reality in detail last week, but here’s a brief refresher. There’s broad sentiment that specialists pay is too high and primary care pay is too low. Many, including the head of CMS, believe that dynamic needs to change. The truth is, it already has.
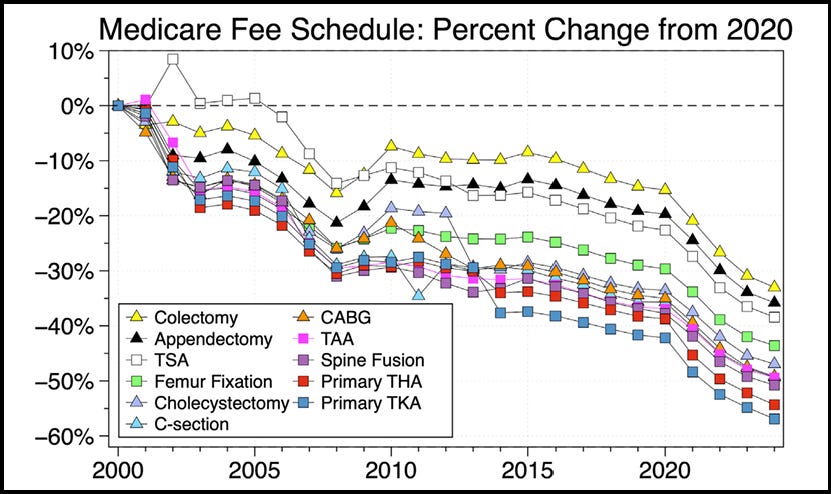
The short version is that inflation-adjusted Medicare reimbursement for joint replacements has declined 57% over the last 20 years. Other surgical specialties have experienced similar, though less severe, declines (Figure 1). The 2026 Medicare Fee Schedule included an across the board 2.5% efficiency cut for almost all procedures.
You could argue that CMS is effectively "taxing" the perceived efficiency of surgeons to subsidize the "cognitive time" of primary care. The point here is not to fall into the unhelpful specialists v. PCPs compensation debate. That’s a relic of budget neutrality, not sophisticated, innovative care models. As an aside, I’d argue the two should be decoupled entirely.
The more important point is that perpetuating the tug-of-war between primary and specialty care is probably counterproductive to CMS’ goals. You don’t foster collaboration by putting your thumb on the scales. Nor do you derive value by creating an accountability trap that catches patients in the middle.
The Accountability Trap
CMS wants all beneficiaries in some form of accountable care by 2030 — a goal that has persisted across administrations. Since its inception 20 years ago, CMMI has spent significant time and resources building accountable care architecture. Despite an uneven start, the numbers are starting to support the thesis. Moving away from fee-for-service towards outcome-based accountability feels right, no argument there. But the structure seems off.
The Logic
The premise of the argument goes something like this:
Specialty care is expensive
Avoiding specialty care decreases costs
The best way to avoid specialty care is to shift accountability (i.e., control) away from specialists
Corollary: Taking accountability away from specialists forces collaboration
This thesis is reflected throughout recent CMMI models. For example, ACO LEAD is primary care-led by design. Specialists participate as Preferred Providers through CARA which turns ACOs into conveners (with CMS’ help). Meanwhile, specialists take on episode-based financial risk with less data access and less organizational authority than the ACO creating their benchmarks. ACOs might be accountable for the total cost of care, but what happens when their upstream decisions skew downstream results?
LEAD isn’t the only program that attempts to preempt specialists. ACCESS addresses chronic MSK conditions but routes intervention through technology platforms. TEAM and CJR- X place accountability at the health system level. The common thread in all these programs is the lack of explicit specialist leadership.
This subversion of specialty leadership contradicts the evidence. A JAMA analysis of 91 orthopedic groups in BPCI Model 2 found reduced Medicare payments and improved clinical outcomes with no change in patient complexity. Savings came from reduced utilization of postacute services (SNF discharge rates, home health utilization, readmissions) — postop care decisions best driven by specialists.
Another study found that physician group practices saved $240 more per BPCI-A episode than hospitals. Surgeons were also more likely to participate even though the model was voluntary. The authors presciently concluded that “future models should consider strategies to align physicians when participation is restricted to hospitals.” That restriction is occurring now; the alignment isn’t.
If specialists perform well when held accountable why cut them out of the loop?
Who Watches the Watchers?
The working assumption throughout these models is that shifting accountability away from specialists will lower costs and drive better decisions. But data are only as useful as the person interpreting it. If your LEAD dashboard shows a 20% SNF discharge rate post joint replacement, should it be up to a primary care ACO to determine whether that's appropriate and acceptable?
Who can distinguish a risk stratification problem from a surgical quality problem from a post-acute management problem? Who identifies which surgeons are cherry-picking healthy patients and which are managing a genuinely complex population? Who manages edge cases that don’t fit neatly into defined appropriateness criteria?
Does such a person exist in primary care-led ACOs?
Don’t get me wrong. There are certainly situations in which MSK conditions can be appropriately evaluated and managed by non-specialists. But how do you make that determination and who’s best to make it? What’s best for the patient? We universally agree that non-specialist medical directors working for payers shouldn’t be making specialty care UM decisions. Why accept that same mechanism inside a VBC program?
Payment model doesn’t change accountability or clinical rigor, nor should it.
[Sidebar: AI is a possible solution to close this gap, but using AI to upskill PCPs doesn’t solve the fundamental problem. AI or not, do PCPs want to be accountable for specialty level care? Should specialists be accountable for the consequences of those decisions?]
Collaboration: Theory v. Reality
CMS seems to believe that collaboration is the answer to the accountability problem. Collaboration sounds great in theory. In an ideal world, PCPs and specialists would closely co-manage patients to reduce fragmentation and gaps in care. But collaboration isn’t what it used to be.
PCP and specialist collaboration has degraded for a variety of reasons — employment and consolidation of PCP groups, siloing of care, and EMR-driven inefficiencies to name a few. Tech can foster collaboration, but inbox fatigue and the “garbage in, garbage out” remain. Frontline reality is that many physicians, specialists and PCPs alike, simply don’t have the time or bandwidth for meaningful, consistent collaboration. Years of self-inflicted structural and systemic wounds led to this point. Payment models won’t lead us out.
Unfortunately, collaboration simply doesn’t happen in the real world to the level it should. Incentivizing collaboration through payment model design risks making it another gameable metric that sounds good in theory but ends up perfunctory in practice. Ideally, you’d fix the underlying structural problems that made collaboration so difficult in the first place.
Lessons from BPCI
CMS seems to believe that accountability works best when shouldered by PCPs. What if the inverse were equally true? What if specialists also take accountability for whole-person care? What happens when specialty care becomes the entry point for prevention and chronic care management?
What if we already had the answer?
Staying in Your Lane
BPCI taught us important lessons in accountability. Orthopedic Surgeons quickly learned that improving a patient’s overall health was a critical component of bundle success. BPCI made it no longer acceptable to cut first and worry about the consequences later. Specialists now had to consider the entire patient and the impact of social drivers, mental health, and other holistic factors.
That didn’t mean Ortho Surgeons started managing blood sugars or titrating hypertension meds. Instead, many hired nurse navigators, established preoperative optimization clinics, and developed surgical appropriateness guidelines. Rather than gatekeepers, surgeons became traffic cops, identifying modifiable risk factors then guiding patients to the proper experts.
Orthopedic Surgeons didn’t try to route patients away from primary care. In fact, they did the opposite — identifying undiagnosed or undertreated medical conditions and making sure patients followed up with the people most qualified to address them. No one, including the surgeons themselves, thought Orthopedists managing chronic medical conditions was the best thing for patients.
Shouldn’t the reverse be true for PCPs and chronic MSK conditions?
Inversion
Another lesson of BPCI was that MSK conditions are often the canary in the coal mine of declining overall health.
High blood pressure, poorly controlled blood sugars, and early-stage renal failure don’t necessarily drive people to seek medical care. Painful backs and joints do. Specialty care as a gateway to primary care is a hidden inversion that can be leveraged in powerful ways.
A patient with bone-on-bone knee arthritis who wants their life back will lose weight, stop smoking, and get their diabetes under control if you make it a condition of safer, lower risk surgery. Though optimization isn’t a panacea, research shows that some lifestyle changes and health benefits persist.
Patients who manage to stop smoking before surgery are more likely to remain smoke-free after surgery. Similar benefits are seen with perioperative glycemic control. Persistent weight loss is trickier; most patients either stay the same or gain weight after surgery. However, studies specific to weight loss as part of an optimization program are lacking. Still, favorable non-MSK disease management outcomes can be achieved through the leverage point of an elective procedure.
This inversion should be harnessed, not ignored.
Thinking Again
CMS is spending enormous resources on chronic disease prevention programs to move needles that well-designed preoperative optimization protocols already move. Specialists aren’t the problem in the cost equation. In the right model, they’re one of the most underutilized chronic disease management assets in the Medicare system. Dell Medical School’s Musculoskeletal Institute and the Joint Health Program at Duke Margolis are examples of specialist-led whole health can be.
The question isn’t whether PCPs or AI can manage some MSK conditions in some patients. They probably can. The question is who’s best positioned to make that determination and who should be accountable for the consequences when they get it wrong.
CMS keeps building accountability mechanisms that separate financial risk from clinical authority. Programs like ACCESS, ACO LEAD, CJR-X, and TEAM let someone else control the levers while specialists absorb the downside. They limit specialist leadership opportunities while relying on the false premise that specialty care avoidance equates to value.
That theory might be right. It could also be a costly mistake.
Next week in Part Two: a way out of the accountability trap, why CMS’ current approach isn't quite right, and the Ambulatory Specialty Model.
Ben Schwartz, MD, MBA
Editor-in-Chief

I think you and I live through the same time of orthopedic care. You couldn’t be more correct. Your words were strong and clear. Well said.
Such a fantastic and insightful article. I've seen this problem of specialist deprioritization become pervasive in CMS models. Some of these wounds are self-inflicted, though. I've spent the last five years crying from the rooftops trying to get our orthopedic surgeon colleagues to learn more about value-based care and be willing to adopt care navigation pathways upstream or embrace stratification. When confronted with these models, a lot of us ask, "Are there RVUs for this?". And I do blame the opacity and reluctance around gainsharing arrangements from incumbents, in part, for this. People respond to incentives, and seems like ours keep getting stripped away. However, I really think that we as orthopedic surgeons need to organize ourselves and become much more savvy around things like the upcoming CMS-administered risk arrangements. We've been dealt some crummy cards, but I'd like to think of myself as a pretty good poker player. We should go all in. Aggregating our expertise and showing concerted efforts to succeed in these models could get us a seat at the table. BTW RevelAi has been selected for the CMS Access Model Program as an ACCESS participant. We are eager to partner with orthopedic surgery groups as "co-managers" in name, but as future quarterbacks for these models in practice.